EMERGENCY MEDICAL SERVICES (EMS) AGENCY-CE26
ECG of The Month —January 2023
Case:
Paramedics respond to a 52-year-old female with a history of hypertension and diabetes, presenting with weakness, nausea, and chest pressure. She has “felt bad” since eating dinner a few hours ago and thinks it may be food poisoning. The patient is diaphoretic and appears to be in distress. Vital signs are BP 138/84 HR 62 RR 18 SpO2 98%.
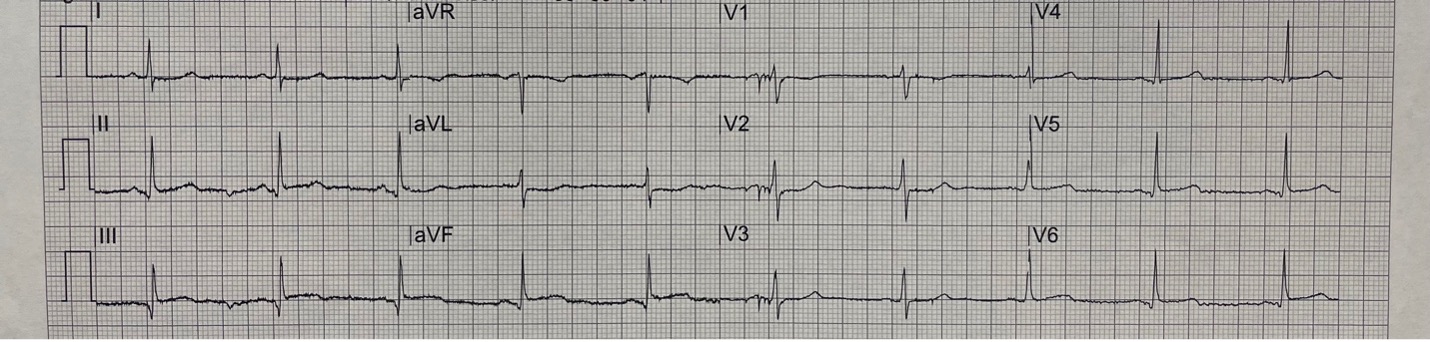
Rate: 60 bpm
Rhythm: Sinus Rhythm – there are p waves before each QRS
ST Segment Elevation >1mm
In 2 or more contiguous
Leads?: No, however there is ST elevation < 1mm in leads III and aVF
Reciprocal Changes: There is slight ST depression in leads I and aVL
This ECG, along with patient presentation, is concerning for acute coronary syndrome. Even though the initial ECG does not have > 1mm ST elevation in 2 or more contiguous leads, there is slight elevation in the inferior leads (II, III and aVF) with reciprocal changes in the lateral leads (I and aVL). This can be a sign of an evolving STEMI. Coronary artery occlusion leads to ST elevation, but early findings may be subtle. A repeat ECG is warranted and may demonstrate a STEMI. A tool to remember where to look for reciprocal changes is the “PAILS” mnemonic:
Posterior → Anterior reciprocal changes
Anterior → Inferior reciprocal changes
Inferior → Lateral reciprocal changes
Lateral ⇔ Septal or Inferior reciprocal changes (exception to the rule, can go in either direction)
Septal → Posterior reciprocal changes
This patient is having cardiac chest pain due to a suspected inferior myocardial infarction though definitive ST elevations are not yet apparent. The initial provider impression would be Chest Pain Suspected Cardiac. Treatment would be in accordance with TP 1211 – Cardiac Chest Pain. Administer Aspirin 325mg chewable tablet PO. Treat pain with Nitroglycerin 0.4mg SL and opioids if indicated. Note that the ST changes suggest an evolving inferior myocardial infarction, but because the patient is normotensive, she can receive nitroglycerin (as stated in TP-1211, special consideration 4, inferior myocardial infarction alone is not a contraindication).
The ECG should be repeated since her presentation and past medical history put her at risk for myocardial infarction and there should be a high clinical suspicion for an evolving STEMI. It is appropriate to discuss destination with the Base hospital given this concern.
A repeat ECG is shown below:
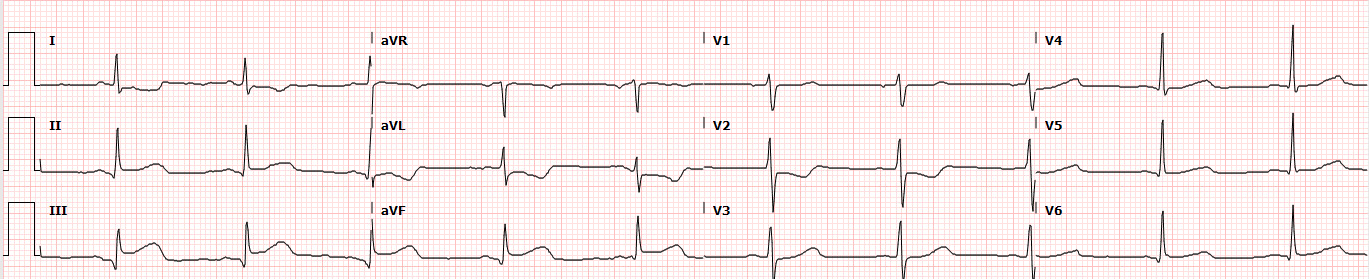
Figure 2. A repeat ECG demonstrates an evolving inferior STEMI. Note the ST elevations now present in lead II, III, and aVF. The reciprocal ST depressions in leads I and aVL are now more prominent.
The provider impression is now Chest Pain STEMI. Initiate ECG transmission and notify the closest STEMI Receiving Center (SRC) as soon as STEMI is identified in accordance with MCG 1303. Transport the patient to the closest SRC.
References
Author: Denise Whitfield, MD, MBA
