EMERGENCY MEDICAL SERVICES-CE24
ECG of The Month — October 2020
Case Presentation:
Paramedics are called to the scene for a young man, approximately in his late 20’s, who was found minimally responsive at his residence by his roommate. Upon arriving on scene, the patient is warm to touch. Initial vital signs are Temp 102.4, BP 85/40, HR 125, RR 20, SpO2 98%. He has dilated pupils bilaterally. There are multiple open pill bottles at the scene including ibuprofen, amitriptyline, and loratadine. You obtain this ECG in the field.
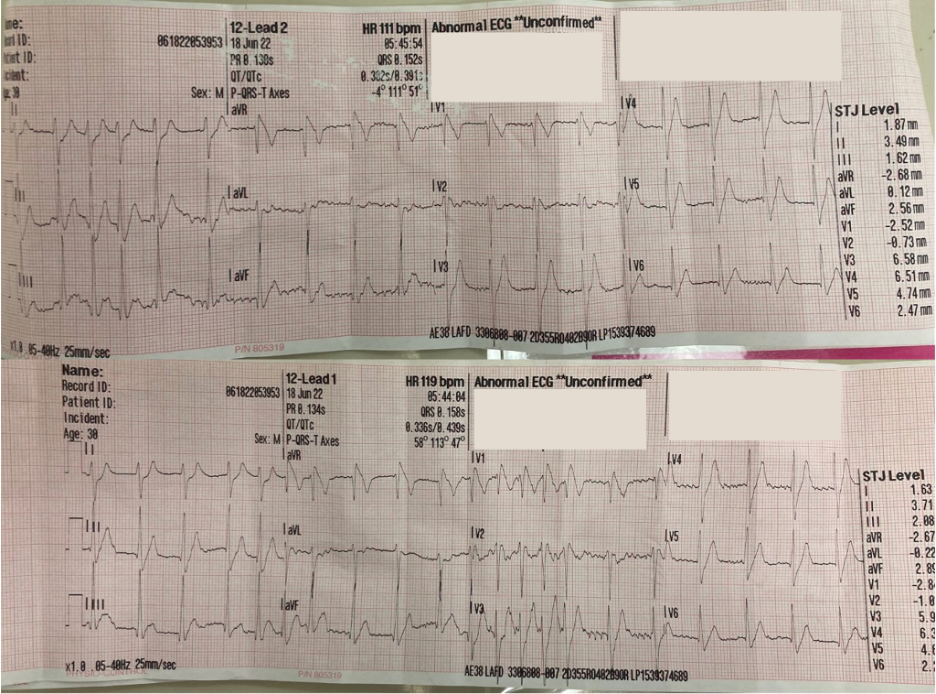
Rate: Variable, between 100-150
Rhythm: Primarily sinus tachycardia with paroxysmal supraventricular tachycardia lasting up to 6 beats.
ST Segment Elevation >1mm
In 2 or more contiguous
Leads?: No
Reciprocal Changes: None
Other: QRS prolongation with a terminal R wave in aVR
This ECG demonstrates a number of abnormalities that correlate with acute sodium channel blockade as seen in several drug toxicities, including tricyclic antidepressant (TCA) overdose.
The standard features of sodium channel blockade are: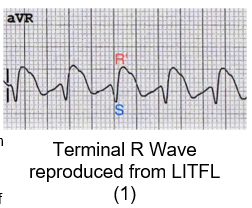
- a prolonged QRS > 100ms
- a measured terminal R wave in aVR measuring > 3mm
- sinus tachycardia
These changes are seen due to the mechanics and kinetics of drugs binding to the activated sodium channel within the heart.
In a normal patient, a cardiac action potential occurs in a four-phase process.
- Phase 0 encompasses the initial depolarization of the cardiac membrane with rapid influx of sodium through opening of voltage-gated channels.
- Phase 1 is the initial repolarization of the cardiac membrane through the opening of potassium and calcium channels. Together, these first two phases determine the QRS complex.
- Phase 2 is an isoelectric phase where there is a balance between potassium ions leaving the cell and calcium ions entering the cell which corresponds to the ST segment of the standard ECG.
- Phase 3 corresponds to continued release of potassium ions and the repolarization of the cardiac membrane which we recognize as the T wave.
- Phase 4 is an isoelectric phase where the cardiac cell returns to its resting membrane potential and is ready to receive a signal for another depolarization.1
In sodium channel blockade, there is selective blockage of activated sodium channels which results in prolongation of Phase 0, the initial depolarization. As a result, the influx of sodium is reduced, resulting in a prolonged QRS.
It is typically thought that the right ventricular conduction system is more sensitive to the effects of sodium channel blockade. The specific result of this in sodium channel blockade is that you will see a prolonged depolarization of the right side of the heart which manifests as a right axis deviation with a dominant R wave in aVR on ECG. Similarly, due to the deviation of the electrical axis within the heart, you will see a deep S wave in Lead I.
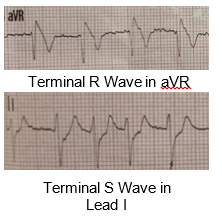
This finding is pathognomonic for sodium channel blockade, one manifestation of tricyclic antidepressant toxicity (TCA) toxicity. Amitriptyline is a TCA and is the likely cause of this patient’s symptoms.
Due to the ability of TCAs to exert anticholinergic, muscarinic, and anti-alpha adrenergic effects, these patients may present with hypotension or signs and symptoms of an anticholinergic toxicity with hyperthermia, flushed skin, pupillary dilation, delirium, urinary retention as well as tachycardia.3 TCA overdose patients are at increased risk for complications including seizures, hypotension, and cardiac dysrhythmia.
This is an acutely ill and hypotensive patient who will require immediate field intervention by EMS. Based on his presentation, this patient should be managed according to TP-1241, Overdose/Poisoning/Ingestion and TP-1213, Cardiac Dysrhythmia – Tachycardia. EMS should establish vascular access and start Normal Saline 1L IV/IO rapid infusion, for the patient’s sinus tachycardia with poor perfusion. Often, in these patients, hypotension is refractory to fluids, and signs of shock will not improve with fluid bolus alone (the hypotension is mediated by drug-induced blockade of alpha receptors on the vasculature). Reversal of the drug induced blockade is needed which is the rationale for giving Sodium Bicarbonate as a treatment.
A 12-lead ECG should be obtained with recognition of ECG findings consistent with sodium channel blockade which can be caused by many drugs including TCA overdose. It is recommended to keep the ECG leads on the patient for repeat ECGs during transit. Per TP-1241, Overdose/Poisoning/Ingestion contact the Base Hospital to discuss antidote administration. Recognition of the ECG pattern will facilitate early field treatment. The patient should receive Sodium Bicarbonate 50 mEq (50mL) IV pushed over 60 seconds for suspected TCA overdose given the empty bottle of amitriptyline at the scene. Often, these patients may need repeat doses of sodium bicarbonate as directed by the Base Hospital with an aim to reduce the QRS below 100 ms.
Patients who experience seizure should be treated promptly as per TP-1231, Seizure with Midazolam 5mg (1mL) IV/IO with repeat given x1 in 2 minutes prn and Base Hospital should be contacted for further dosing as indicated. This is important as seizures increase the acidosis a patient may experience which may increase the binding of some sodium channel blocking agents to the channel and worsen the effects leading to rapid decompensation.
The history of likely ingested substances should be brought to the attention of the Emergency Department, and one may consider contacting the Poison Control Center (1-800-222-1222) in conjunction with the Base for assistance with identification and management of unknown drugs.
These patients are at high risk for decompensation with cardiac dysrhythmia and EMS providers should be prepared to initiate resuscitative measures per TP-1210, Cardiac Arrest.
The patient remained hypotensive during transit despite fluid resuscitation and sodium bicarbonate administration. During his time in the emergency department, he became acutely tachycardic to the 180s, and started seizing. He was treated with benzodiazepines for seizures and additional sodium bicarbonate was administered. The patient was intubated for airway protection. Despite all resuscitation efforts, the patient went into cardiac arrest and died in the emergency department.
Author: Jonathan Warren, MD; Denise Whitfield, MD, MBA
References:
- Costanzo, Linda. (2014). Physiology (5th edition). Elsevier. Pg. 129-133
- Rengasayee Veeraraghavan, Steven Poelzing, Mechanisms underlying increased right ventricular conduction sensitivity to flecainide challenge, Cardiovascular Research, Volume 77, Issue 4, 1 March 2008, Pages 749–756, https://doi.org/10.1093/cvr/cvm090
- Farkas, Josh, Sodium Channel Blocker Toxicity (including tricyclic antidepressants), 2021 Apr 26; accessed 2022 Sept 10. https://emcrit.org/ibcc/nacb/
Image Sources:
- https://litfl.com/tricyclic-overdose-sodium-channel-blocker-toxicity/
- https://commons.wikimedia.org/wiki/File:Cardiac_action_potential.svg
- https://commons.wikimedia.org/wiki/File:Action_potential_class_Ic.svg
Author: Jonathan Warren, MD; Denise Whitfield, MD, MBA

{kind=link}
{kind=link}