EMERGENCY MEDICAL SERVICES-ECG August Issue
Case:
Paramedics respond to a 59-year-old female with weakness and left jaw pain. She was gardening outside when she suddenly felt nauseated and weak. Her vital signs are BP 156/94 HR 72 RR 16 O2Sat 98%
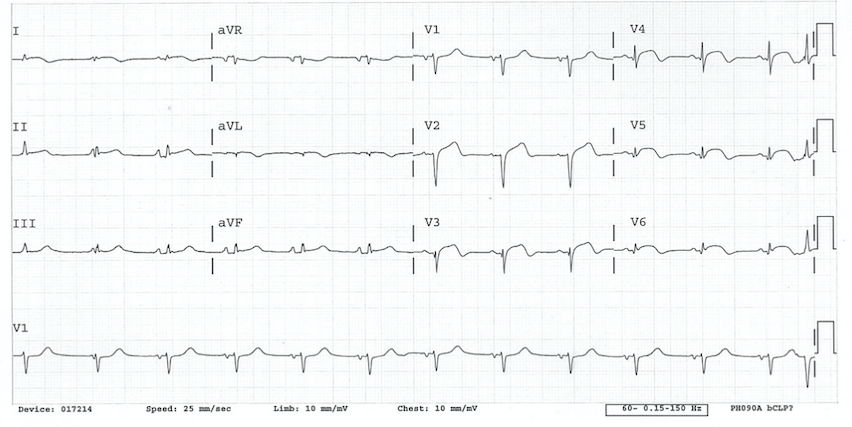
Rate: ~80 bpm
Rhythm: Normal Sinus Rhythm (there are p-waves before each QRS)
ST Segment Elevation >1mm
In 2 or more contiguous
Leads?: Yes. There is ST elevation in precordial leads V2-V6.
Reciprocal Changes?: No reciprocal changes are seen in the inferior leads
This ECG is consistent with an antero-lateral STEMI. The ECG has ST elevation in the anterior (V2-V4) and lateral (V5,V6) leads with developing ST elevation in lateral leads I and aVL.
The anterior and lateral wall of the heart are supplied by the left anterior descending (LAD) and left circumflex (LCx) arteries. Depending on the anatomical location of the occlusion, lateral infarctions can have different ECG patterns. A proximal lesion to the LAD can impede flow, leading to an infarction to the anterior and lateral portions of the heart. A proximal LCx lesion also supplies both the anterior and lateral portions of the heart and can lead to a similar pattern depending on individual anatomy, but could also involve the inferior, lateral and posterior portions of the heart. Isolated lateral infarctions are typically due to occlusions in smaller branch vessels. In lateral STEMIs, reciprocal depressions in inferior leads II, III and avF can be seen when there are ST elevations in I and aVL. Reciprocal changes will not be seen if the infarction extends into the inferior portion of the heart (concomitant inferior ST elevation in an inferolateral STEMI).
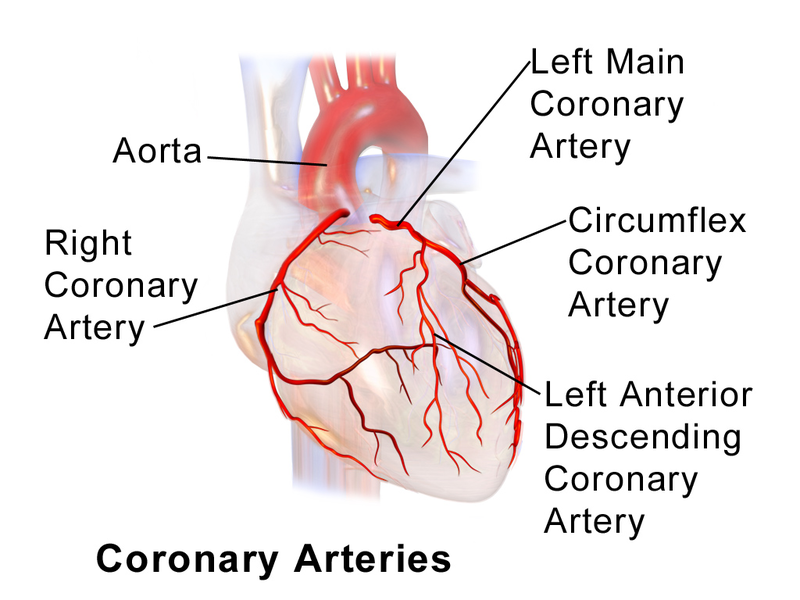
Figure 1. Coronary artery anatomy. The left anterior descending (LAD) and left cirumflex (LCx) coronary arteries supply the antero-lateral portion of the heart. Source: https://commons.wikimedia.org/wiki/File:Blausen_0256_CoronaryArteries_02.png
Women may have atypical clinical presentations when having a myocardial infarction. Although chest pain remains the most common presenting symptom for myocardial infarction in women, the absence of chest pain does not exclude myocardial infarction. This patient has concerning symptoms of nausea, weakness and jaw pain which can all be presenting symptoms for myocardial infarction. Pain caused by coronary artery occlusion can be in the chest but may also be referred to the shoulder or jaw. This can lead to confusion as to the cause, but whenever jaw or shoulder pain are seen, based on full assessment and presenting age, signs and symptoms, and past medical history of the patient, cardiac chest pain must be considered.
Although her chief complaint is not “chest pain”, this patient is having a STEMI and should be managed in accordance with TP-1211, Cardiac Chest Pain. It is most important to recognize the signs of a heart attack, especially when they are atypical, and obtain an ECG. The patient should receive Aspirin 325g, Nitroglycerin 0.4mg SL for her jaw pain, which is referred anginal pain, and ondansetron 4mg ODT prn for nausea. The ECG should be transmitted to the STEMI Receiving Center (SRC) and the patient transported to the SRC after notification.
This patient was transported to the SRC where she underwent immediate cardiac catheterization. A stent was placed in her LCx artery with successful reperfusion and she was discharged 2 days later.
References
- Burns E, Buttner R. Lateral STEMI. LITFL. https://litfl.com/lateral-stemi-ecg-library/ Accessed August 16, 2021.
- Lawesson S, et al. Gender differences in symptoms presentation of ST-elevation myocardial infarction – an observational multicenter survey study. Int J Cardiol. 2018;264:7-11.
Author: Denise Whitfield, MD, MBA
