ECG OF THE MONTH- April 2024
Case Presentation:
Paramedics respond to a 42-year-old female with dizziness, chest tightness, and shortness of breath. Her symptoms started about 30 minutes prior to EMS arrival while she was jogging. Her spouse called 911 because she “didn’t look right and seemed anxious.” Initial vital signs on scene are BP:132/61 HR: 95 RR: 20 SpO2: 99%.
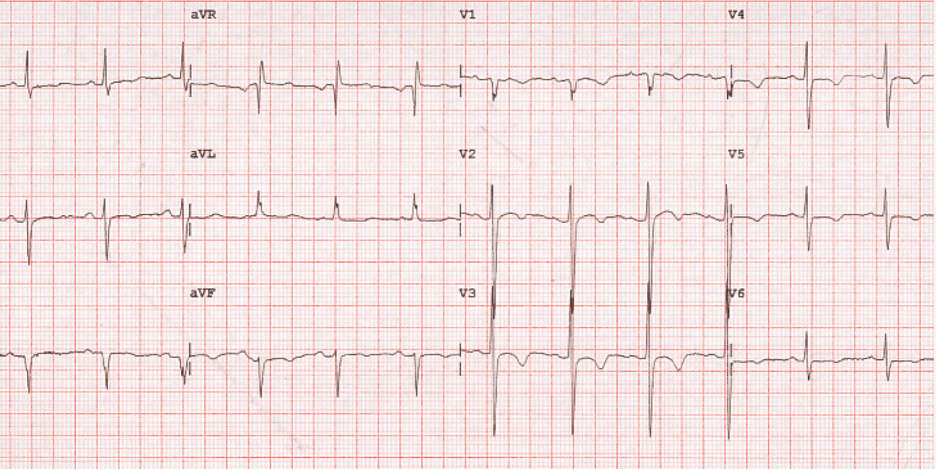
Rate: ~90 bpm
Rhythm: Normal sinus rhythm. There is a p wave before every QRS complex.
ST Segment Elevation >1mm
In 2 or more contiguous
Leads? No
Ischemic Changes: ST depression and t-wave inversion in the anterior/lateral leads (I, aVL, V2-V6).
This ECG suggests myocardial ischemia. There are ST segment depressions and t-wave inversions in contiguous leads (lateral – I, aVL, V5, V6; anterior – V2-V4). Though not a STEMI, non-ST elevation acute coronary syndromes are cardiac emergencies that should be recognized by EMS clinicians. The patient is experiencing ischemia to the heart and requires emergent inpatient hospital management.
Acute coronary syndrome is a catch all term that refers to syndromes resulting from acute blockage (“occlusion”) of coronary vessels. Prehospital clinicians often focus on recognizing STEMI, because this determines destination routing to a SRC for emergency cardiac catheterization. Patients can have myocardial infarction (“heart attacks”) that do not have ST elevation, known as non-ST Elevation Myocardial Infarction (NSTEMI). These patients typically “rule in” for a myocardial infarction with emergency department laboratory studies (i.e. troponin). While patients with NSTEMI do not go to the cardiac catheterization lab immediately like STEMI patients, they typically require medical management and cardiac catheterization during their hospital admission.
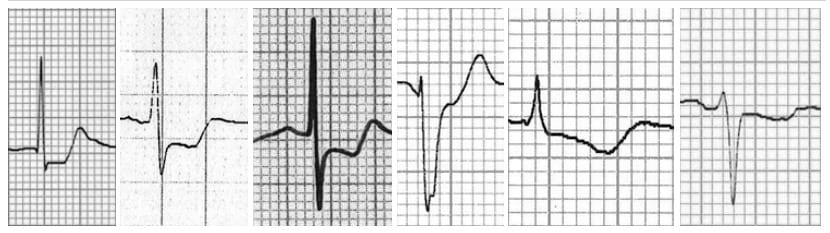
Figure 1. Examples of ST segment depression in myocardial ischemia. Image Source: LITFL https://litfl.com/wp-content/uploads/2018/08/ST-segment-morphology-in-myocardial-ischaemia%EF%BB%BF.jpg accessed 3/25/2024
This patient’s ECG shows signs of cardiac ischemia. Cardiac ischemia/infarction symptoms can present atypically, especially in women. Although this patient does not explicitly describe chest “pain” her dizziness, chest “tightness” and shortness of breath are cardiac symptoms. Chest Pain – Suspected Cardiac is the provider impression and the patient should be managed in accordance with TP – 1211 – Cardiac Chest Pain.
The patient is not hypoxic and does not require supplemental oxygen. ASA 325mg chewable is administered as well as Nitroglycerin 0.4mg SL which improves her pain. She is not a STEMI, so her destination is the MAR. Her evaluation in the emergency department reveals an elevated troponin that rules her in for a NSTEMI. She is admitted to the cardiology service where she receives a cardiac catheterization the next day.
Author: Denise Whitfield, MD, MBA
References
1. Burns E, Cadogan M. Myocardial Ischaemia. https://litfl.com/myocardial-ischaemia-ecg-library/. Accessed 3/25/24.

{kind=link}