EMERGENCY MEDICAL SERVICES-CE29
ECG OF THE MONTH – August 2022
Paramedics respond to a 36-year-old female whose spouse called 911 after the patient lost consciousness. The patient was sitting in her backyard when she suddenly slumped over in her chair and was unresponsive. The episode lasted approximately 20 seconds. She then regained consciousness. She has a history of depression, for which she takes an antidepressant, but is otherwise healthy and denies current depression symptoms. She is awake and alert when EMS arrives.
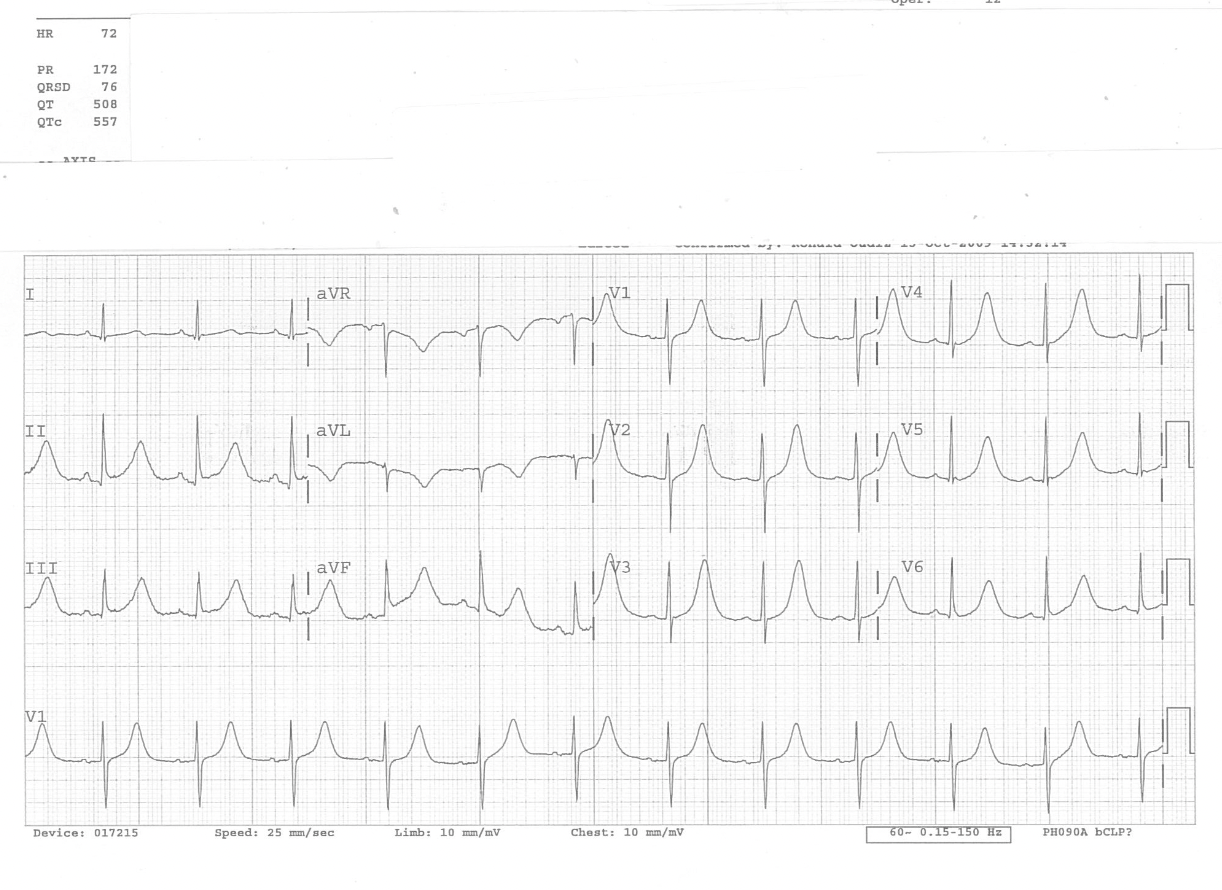
Rate: ~72 bpm
Rhythm: Normal Sinus Rhythm (there are p-waves before each sinus beat QRS)
ST Segment Elevation >1mm
In 2 or more contiguous
Leads?: No
Reciprocal Changes: N/A; a nonspecific t-wave inversion is present in lead aVL
Other: QT = 508ms; corrected QT (QTc) interval = 557ms
This ECG demonstrates a prolonged QT/QTc interval. The QT interval is defined as the time from the start of the Q wave to the end of the t-wave.
The QT interval represents the time from the onset of ventricular depolarization to the end of ventricular repolarization, which correlates to the time of ventricular systole from ventricular contraction to ventricular relaxation. The QT interval shortens at faster heart rates and lengthens at slower heart rates. To standardize comparison across varying heart rates, the QTc is calculated to provide an estimate of the QT interval at a heart rate of 60bpm. A prolonged QTc is an established risk factor for developing Torsades de Pointes, a malignant ventricular arrhythmia that can deteriorate into ventricular fibrillation.
The QTc can be calculated using several formulas. However, most ECG machines calculate the QTc and display the calculation in the machine ECG interpretation.
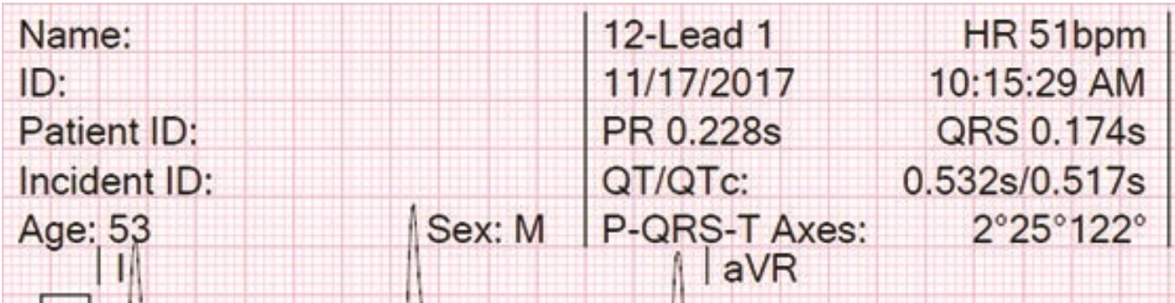
Figure 2. The QT/QTc is typically calculated and presented in the ECG machine interpretation.
Another way to estimate QT prolongation is comparing the QT interval with the R-R interval; the QT interval should be less than half the duration of the preceding R-R interval.
A QTc is considered prolonged if >440ms in men or >460ms in women. A QTc > 500ms is associated with an increased risk of Torsades de Pointes, a malignant ventricular dysrhythmia that can be asymptomatic but is also associated with syncope or sudden death. Torsade de Pointes, a term meaning “twisting of the points”, appears on ECG as a polymorphic ventricular tachycardia that oscillates in amplitude. It may resolve without intervention, persist, or deteriorate to ventricular fibrillation.
A prolonged QT interval can be caused by many factors. Some individuals have genetic causes related to their cardiac ion channels that result in QT prolongation, known as long QT syndrome. Other common acquired causes include electrolyte abnormalities, cardiac ischemia, hypothermia, and certain medications. In Los Angeles County EMS protocols, ondansetron is a QT prolonging medication. Olanzapine will be introduced October 2022 and is QT prolonging as well; for this reason, coadministration of these two medications is contraindicated.
This patient presented with a syncopal episode and was found to have a prolonged QT interval on ECG. Treatment should be in accordance with TP 1233 “Syncope / Near Syncope”. The patient should be monitored for cardiac dysrhythmia during transport. A prolonged QT interval is a risk factor for Torsades de Pointes which can result in ventricular fibrillation and sudden cardiac death. The patient needs to be transported by paramedics to the most accessible receiving facility (MAR) for further evaluation. If the patient develops a ventricular tachydysrhythmia, treat in accordance with TP 1213 “Cardiac Dysrhythmia – Tachycardia”. Should Torsades de Pointes develop, treat as per TP 1213 wide complex-irregular tachycardia.
The patient was transported to the MAR where the patient was admitted for further cardiac evaluation. On further history, it was determined that she has been taking a long-standing antidepressant medication (citalopram) and recently started on an antibiotic (levofloxicin). The antibiotic was discontinued, and her QT interval returned to normal.
References
- Burns E, Buttner R. QT Interval. Life in the fast lane. 20 https://litfl.com/qt-interval-ecg-library/ Accessed July 25, 2022.
- Beach SR et al. QTc prolongation, torsades de pointes, and psychotropic medications. Psychosomatics. 2013;54(1):1-13.
- Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart. 2003; 89(11): 1363-1372.
Author: Denise Whitfield, MD, MBA
